 The final countdown has begun. In a few short days I and the rest of the Chilmark Research team will make our annual pilgrimage to the big health IT confab, HIMSS17, to rub shoulders with some 45,000 of our closest friends.
The final countdown has begun. In a few short days I and the rest of the Chilmark Research team will make our annual pilgrimage to the big health IT confab, HIMSS17, to rub shoulders with some 45,000 of our closest friends.
I have a love-hate relationship with this event. I love the opportunity to meet with many leading advocates, innovators, developers, and users of IT who are all truly trying to improve the delivery of care – to improve the patient experience. This is my/our tribe. These individuals and even organizations are who we as analysts seek out, looking to have an in-depth conversation. These conversations are enlightening, help us further refine our research agenda, and provide us the opportunity to accurately report on exactly what is working and, frankly, what may still be more vaporware than software.
HIMSS is not all sweet-smelling roses. What frustrates me the most is the hype. Now I know that vendors pay a pretty penny to exhibit their wares at HIMSS and, having been on the other side of the fence, I know intimately the challenges of trying to differentiate yourself from all the others that surround you. But what I truly hate is when the latest fad or buzzword enters the hype-cycle and every single vendor claims to have that solution, to address that buzzword du jour.
Years ago I remember walking by booth after booth of vendors claiming they had a Health Information Exchange (HIE) solution. When I saw such proudly displayed in the Dell booth, I knew it was all BS and decided to separate the wheat from the chaff with our first report on the HIE market. That report was a huge success and really put wind in the sales of what was then a very small company. In recent years it has been population health management (PHM), a misnomer if there ever was one. Until the last 12-18 months, not a single vendor has been capable of fully supporting an organization’s PHM strategy. There are simply too many moving parts to PHM. Simplistic care gap analysis with robo-emails and calls is not PHM. The sad thing is, these buzzwords get so over-used, so misconstrued, and so abused that they become meaningless – I’m coming close to detesting the term PHM.
Enough of a preamble. The following is what I will be on the lookout for at HIMSS – and you should, too.
1. Artificial intelligence (AI) is big, everywhere, but are we truly seeing traction? This term, along with machine learning and cognitive computing, will be on prominent display at HIMSS17. I would not be surprised if this is the top buzzword at HIMSS this year, but what I really want to know is how AI is actually being used. What are the use cases? Where will it scale first (e.g., consumer, clinician, back-office, radiology…)? What impact will it have on existing processes and workflows? How will it impact staffing levels?
2. Precision medicine: Is it real or still theoretical? There’s been a lot of hype on precision medicine the last couple of years but little action. Will be interested to learn how much traction some of the early innovators are getting (NantHealth) and what new entrants (2bPrecise) are planning. Tremendous amount of opportunity here that overlaps some of the current work being done in AI – how will these two come together in the future to improve and optimize the delivery of care for the individual?
3. How will care management and patient engagement merge – who is thinking beyond silos here? A core tenet to effective care management is patient activation and self-care, yet care management and patient engagement solutions remain by and large completely divorced from one another. Who among vendors, providers, and consultants is truly thinking beyond silos and looking to effectively meld care management and patient engagement?
4. Who is using IoT and PGHD at scale? Despite all the talk of health Internet of things (IoT) and patient generated health data (PGHD), our research to date has yet to find an organization that is using IoT and PGHD at scale for remote care monitoring. Sure, there are plenty of pilots, but as one healthcare executive said to me: Its one thing to do such for 100 patients, quite another for 10,000 – we’ve yet to figure out how to scale the workflow across the enterprise and community.
5. Outcome measures, anyone? The focus of quality initiatives (and measures) for years has been on process measures. We are getting to a level of maturity in the industry’s use of IT that we need to be thinking beyond process measures to outcome measures. In a recent briefing, a leading HIT vendor proudly showed how its clients excel at meeting process measures. When asked how these same clients do on outcome measures – well, that was a question the company had no answer for. It’s time we start figuring this out. I want to know who is doing this on a routine basis and for what use cases.
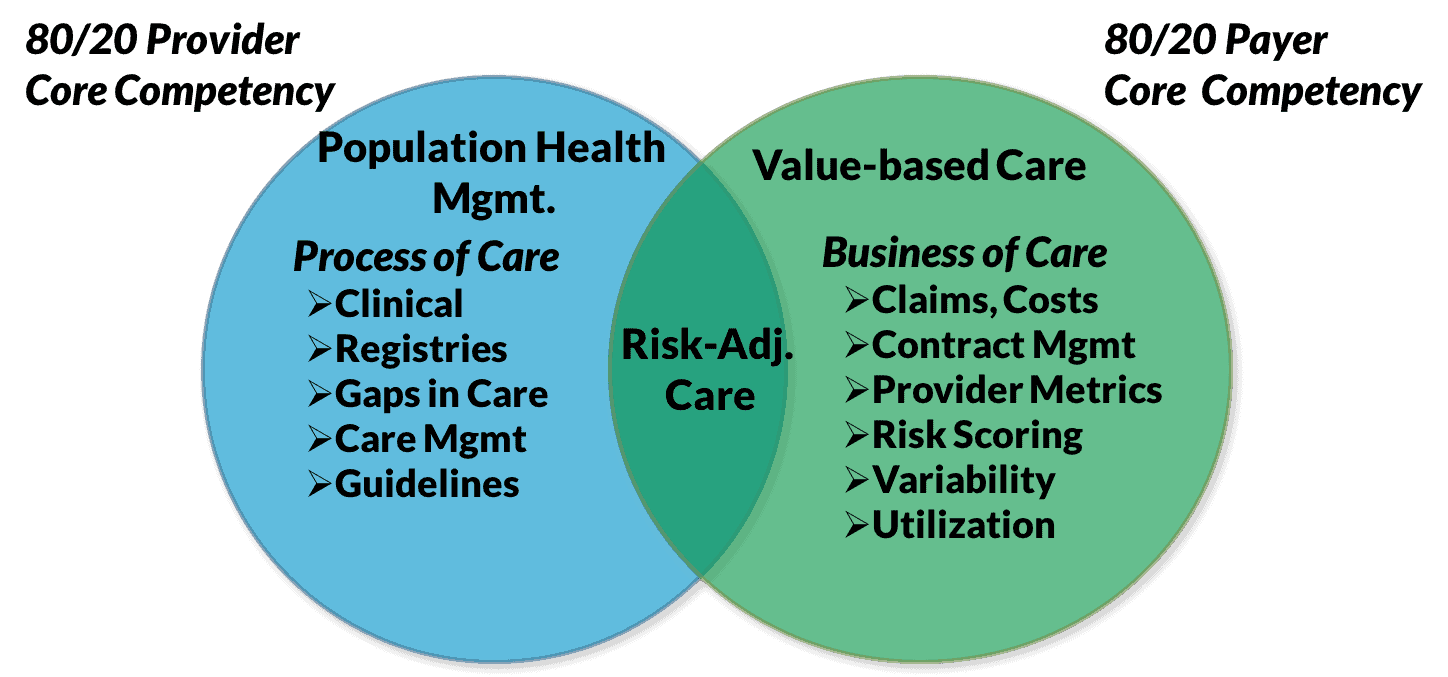 6. How are vendors looking to support PHM and VBC? Core to our research in 2017 is gaining a better understanding of provider-payer convergence. Our thesis is that providers have a core competency in population health management (PHM), whereas payers have competency in value-based care (VBC). As these two entities increasingly collaborate to improve access and care delivery within a community, how will vendors provide a platform to support such requirements?
6. How are vendors looking to support PHM and VBC? Core to our research in 2017 is gaining a better understanding of provider-payer convergence. Our thesis is that providers have a core competency in population health management (PHM), whereas payers have competency in value-based care (VBC). As these two entities increasingly collaborate to improve access and care delivery within a community, how will vendors provide a platform to support such requirements?
7. What’s next? a.k.a., reading the Trump administration tea leaves and what may unfold across the healthcare sector over the next few years. The new administration has made a lot of pronouncements pertaining to healthcare, from pharmaceutical pricing to repealing the Affordable Care Act. We still do not know how all this will play out, and that lack of clarity is likely to impact budgets. I want to know: How big is that impact and how might it impact IT spend going forward? While I can already imagine every vendor telling me that it has a great pipeline, a great backlog, etc., I remain unconvinced. I’ll be digging deep on this one.



0 Comments